Testosterone Injection: Subcutaneous vs. Intramuscular—Where to Inject
Regardless of which TRT product you’ve been prescribed, a common question is where to inject testosterone. For decades, most men have used IM testosterone injections, primarily into the glutes, quads, or deltoids, using a 1 to 1.5-inch syringe. During the past five years, many men have also begun injecting testosterone subcutaneously (SubQ), a shallow injection into the fat layer on the abdominal or other areas—just under the skin but before reaching muscle. Many TRT patients find SubQ injections less bothersome than IM injections, as they require a smaller needle in both length and gauge. SubQ injections are also associated with less irritation for some men with IM injections. While some men may find IM injections to leave a minor soreness at the injected site, SubQ injections cause no noticeable pain or irritation.
Understanding Testosterone Replacement Therapy
Testosterone Replacement Therapy (TRT) is a medical treatment designed to help individuals with low testosterone levels, also known as hypogonadism. TRT aims to restore normal testosterone levels, alleviating symptoms such as low libido, fatigue, and decreased muscle mass. This form of hormone therapy can significantly improve the quality of life for those experiencing sexual dysfunction and other related issues. TRT can be administered through various methods, including intramuscular injections, subcutaneous injections, and topical gels. In this article, we will focus on testosterone injections, specifically intramuscular and subcutaneous injections, to provide a comprehensive understanding of these methods.
Testosterone Injection Methods: Effects on Total Testosterone, Estradiol (E2), and PSA
Testosterone Cypionate and Testosterone Enanthate are the two most commonly used forms of testosterone in men to treat hypogonadism (low testosterone). Both forms carry the same testosterone hormone; the ester is the only difference, which alters the hormone’s time release so that testosterone blood levels can remain up for a few days. These two testosterone compounds are identical in a testosterone replacement therapy (TRT) setting. Both forms are commonly used in hormone replacement therapy to treat hypogonadism in men.
Where and How to Inject Testosterone?
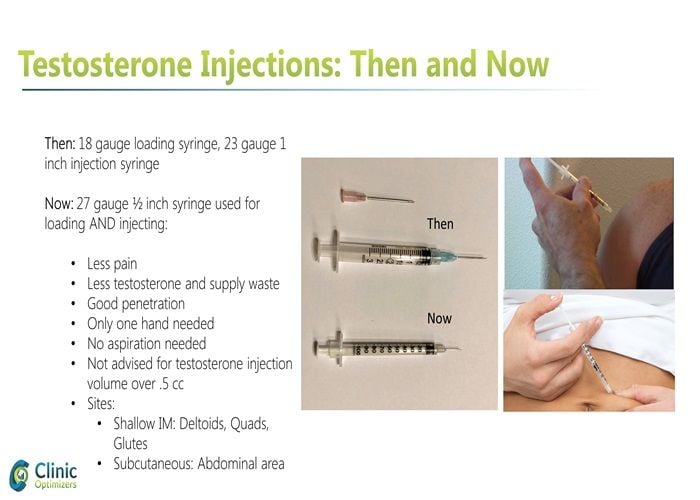
Regardless of which TRT product you’ve been prescribed, a common question is where to inject testosterone. For decades, most men have injected their testosterone intramuscularly (IM), primarily into the glutes, quads, or deltoids, using a 1- to 1.5-inch syringe. During the past five years, many men have also begun injecting testosterone subcutaneously (SubQ), a shallow injection into the fat layer on the abdominal or other areas—just under the skin but before reaching muscle. Many TRT patients find SubQ injections less bothersome than IM injections, as they require a smaller needle in both length and gauge. SubQ injections are also associated with less irritation for some men with IM injections. While some men may find IM injections to leave a minor soreness at the injected site, SubQ injections cause no noticeable pain or irritation. Many patients find it beneficial to inject weekly to maintain stable testosterone levels.
Administering Testosterone Injections Safely
Administering testosterone injections safely requires proper technique and precautions to ensure effectiveness and minimize risks. Before injecting, ensure the injection site is clean and free of any debris. Use a sterile needle and syringe, and follow the recommended dosage and injection frequency as prescribed by your healthcare provider. For intramuscular injections, use a longer needle (1 to 1.5 inches) and insert it at a 90-degree angle into the muscle, typically in the glutes, quads, or deltoids. For subcutaneous injections, use a shorter needle (0.5 to 1 inch) and insert it at a 45-degree angle into the fatty tissue, commonly in the abdominal area. Always dispose of used needles and syringes properly to prevent injury and contamination. By following these steps, you can administer testosterone injections safely and effectively.
Choosing the Right Injection Site
Choosing the right injection site is crucial for safe and effective testosterone injections. For intramuscular injections, common sites include the buttocks, thigh, and upper arm. These areas have larger muscle masses, which are ideal for proper absorption of the hormone. For subcutaneous injections, common sites include the abdomen, thigh, and buttock. When selecting an injection site, consider the following factors:
-
Fat layer: Subcutaneous injections require a sufficient fat layer to ensure proper absorption.
-
Muscle mass: Intramuscular injections require a larger muscle mass to ensure proper absorption.
-
Nerve proximity: Avoid injecting near nerves to minimize the risk of nerve damage.
-
Scarring: Rotate injection sites to minimize scarring and promote even absorption.
By carefully choosing the injection site and rotating locations, you can enhance the effectiveness of your testosterone injections and reduce potential complications.

What is the Best Way to Inject Testosterone?
While subcutaneous testosterone injections are by far the most uncomplicated and most comfortable, the more critical question for any TRT patient is how effective this method is and how it affects the potential adverse side effects of TRT. Weekly injections are often recommended to maintain stable hormone levels and reduce side effects. A recent study from the Department of Urology at the University of California (UC) has provided us with such answers.
The UC study attempted to answer four questions as they relate to IM vs. SubQ testosterone injections:
Comparisons in:
Two hundred thirty-two men took part in the UC study. Baseline levels were recorded for all men in the four measurement areas and then again at 6-12 weeks post-treatment. The results showed that men who underwent SubQ injections of testosterone resulted in a 14% greater increase in total testosterone levels than the testosterone level of IM patients. SubQ patients also had 41% lower hematocrit post-therapy than IM patients and 26.5% lower E2 levels. For both groups of men, there were no elevated levels of PSA.
Additional Studies Comparing IM versus SubQ TRT
While the UC study provides valuable data on four specific lab test values of concern and is one of the most recent studies on the topic of subcutaneous versus intramuscular testosterone injections, it is not the only information we have available. An additional Journal of Clinical Endocrinology study found that normal serum testosterone levels were maintained through SubQ injections. Most patients preferred the injection method due to less injection site pain. Similar results were found in a study headed by Dr. Al-Futais in a Canadian study that ran for one year in 2002.
Similar results for subcutaneous testosterone injections have also been found in female-to-male (FTM) transgender people-based testosterone studies. The Journal of Clinical Endocrinology and Metabolism reported that FTM patients administering SubQ testosterone were found to easily reach stable and normal testosterone levels along with suitable E2 levels. The study concluded that SubQ testosterone injections are both safe and effective. These findings are particularly relevant for those undergoing gender-affirming hormone therapy, as they highlight the effectiveness and patient preference for SubQ injections.
Although far less in-depth than we previously mentioned, a final study of note was published in the Journal of the Endocrine Society. Similar results to the reviews mentioned above were found, along with no significant changes between IM and SubQ patients relating to dihydrotestosterone (DHT). Interestingly, unlike the UC study, this study also measured no notable difference in E2 levels between the two categories. However, it must be noted that this particular study only included a single injection of testosterone undecanoate at 1000 mg.
How to Inject Testosterone Using Subcutaneous Injections?
If subcutaneous testosterone injections are right for you, you will merely need a small insulin syringe to administer the hormone. A 0.5-inch-long, 25-27 gauge needle in a 1 ml syringe will typically suffice. They also do not require aspiration, commonly used in old IM injection techniques. Unlike IM testosterone injections, SubQ injections do not require aspiration and use a smaller needle. Regardless, the aforementioned insulin needles and syringes are your best choice for comfort and ease of use.
Due to the small needle size, you may find it slightly more difficult to draw the testosterone into the insulin syringe. But most men on TRT use 50-100 mg twice per week, which amounts to 0.25 to 0.5 ml of a 200 mg/ml testosterone cypionate or enanthate formulation commonly used in the United States. Those small volumes load up in just 1-2 minutes.
Many TRT clinics prescribe protocols to patients to inject their testosterone subcutaneously once or twice weekly. This protocol effectively maintains stable testosterone levels with small, more frequent doses than the old dose of 200 mg once every two weeks. Two injections that split the weekly dose twice per week will suffice for most patients, such as a Monday and Thursday protocol.
Is There Any Difference Between Testosterone Cypionate and Testosterone Enanthate?
As mentioned early on, testosterone cypionate and testosterone enanthate are the two most commonly prescribed and lowest-cost testosterone esters worldwide. All four studies cited in our discussion were performed using Testosterone Enanthate, excluding the one using Undecanoate. However, using Testosterone Cypionate would have yielded similar, if not identical, results. Both versions of the testosterone hormone are just that, testosterone. Molecularly, there is no difference. It is merely the ester attached, and the carrier oil it may be mixed in is the only difference. Further, as the enanthate and cypionate esters have very similar time-release structures, total serum levels should be relatively the same with either compound, even if injected subcutaneously.
Conclusion
In conclusion, testosterone replacement therapy is a medical treatment designed to help individuals with low testosterone levels. Administering testosterone injections safely requires proper technique and precautions. Choosing the right injection site is crucial for safe and effective testosterone injections. By understanding the differences between intramuscular and subcutaneous injections, individuals can make informed decisions about their treatment options. Always consult with a healthcare professional before starting testosterone replacement therapy to ensure the best approach for your specific needs.
References
How to Inject Testosterone Intramuscularly, Shallow IM, or Subcutaneously?
SIU Academy. Choi E. 10/10/20; 309864; BSP-06.01
Pharmacokinetics and Acceptability of Subcutaneous Injection of Testosterone Undecanoate